
Use of Oxygen resuscitator
Operation of resuscitatorOn board ship, the resuscitation is generally limited to manual resusciators and administering CPR and Mouth-to-Mouth breathing and that does not need equipment, but very good First-Aid training. Ship’s carrying dangerous goods such as LNG/LPG now carries pressurized oxygen and hospital equipment to facilitate such treatment. But this will require also quality medical training to shipboard crew, as part of their competency.
UNITOR: Manual Resuscitator: (bag-valve and mask-resuscitator complete with oxygen reservoir and face masks in 2 sizes) 1 Guedel Airway in 3 sizes, Nebulizer with aerosol mask and oxygen tubing
CPR with resuscitatorOXYGEN ADMINISTRATION AND CONTROLLED VENTILATIONOxygen is necessary for life. Some intoxications may interfere with normal oxygenation of the blood or tissues. In particular, oxygen can be lifesaving to casualties who have inhaled smoke and other toxic gases but it needs to be given with all speed. Basic training is required to administer oxygen.
Diagnosis
- There is difficulty in breathing with an increased rate at first (over 30 per minute). Later it may become slow and stop.
- The pulse is rapid, usually over 100 per minute.
- There is blueness of the skin with purple lips and tongue.
- The casualty may be agitated at first but become apathetic, with muscular weakness. Unconsciousness may follow this.
- The pupils of the eyes will react to light at first. If they become large and do not react to light, life is in danger.
Treatment
- Give oxygen by means of a face mask. It makes assisted or controlled ventilation possible. It is better to have the casualty well oxygenated with controlled artificial respiration than to have him poorly oxygenated from breathing spontaneously.
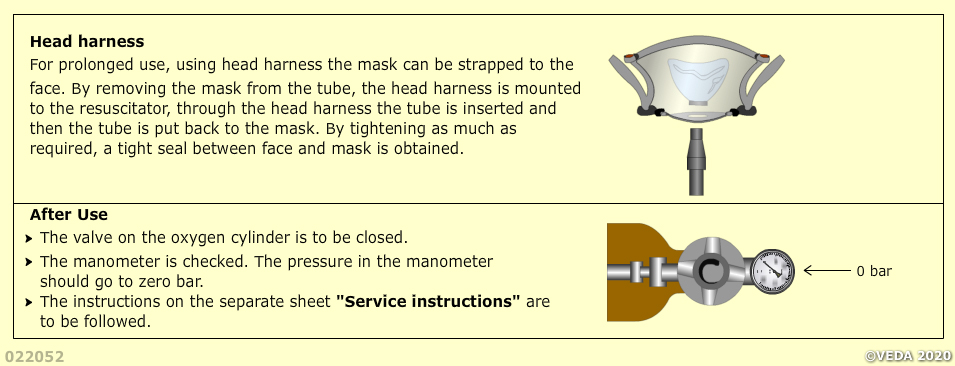
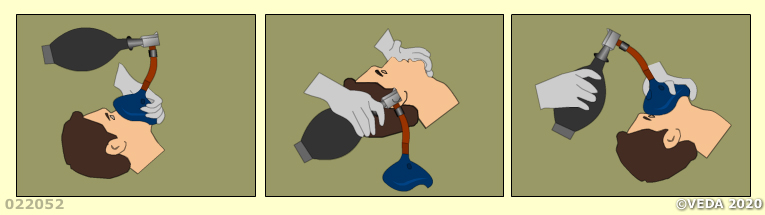
- Place a mask over the nose and mouth. It is essential that the face mask is held firmly in place so as to avoid leakage.
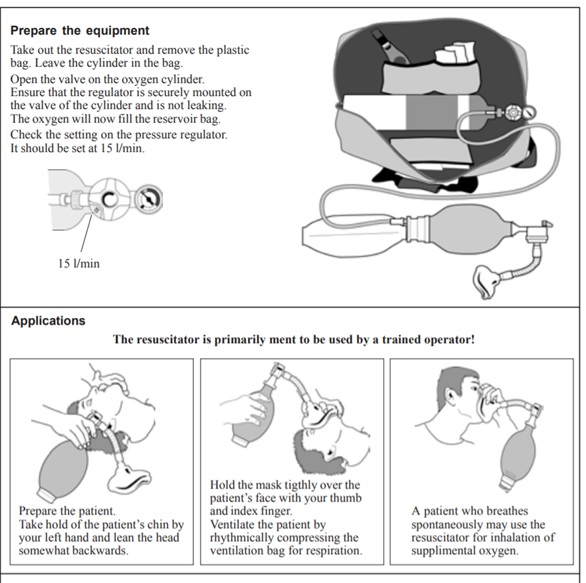
- Check that the equipment is correctly assembled according to the manufacturer’s instructions and that sufficient oxygen is contained in the cylinder (a cylinder of 2.5 litre capacity, filled under a pressure of 200 bar, delivers 500 L oxygen).
The commonest emergency requiring medical assistance on board is toxic gasinhalation from fires or specific toxic gases. Combustion in fires on board may well involve substantial release of carbon monoxide and hydrogen cyanide. In these cases oxygen should be given at a flow rate of 8 L per minute.
In life-threatening conditions, such as lung oedema or circulatory failure, oxygen should also be given at a flow rate of 8 L per minute.
Warning: Smoking, a naked flame or light fires must not be allowed in the same room during the administration of oxygen because of the risk of fire.
In order for a vessel to comply with Column A or B of Appendix 14 of the MFAG the following quantities of oxygen available in the ship’s hospital for resuscitation purposes are required:
- 40 litre@200 bar, medical oxygen cylinder in ships hospital assembled for direct use with 1 flow meter unit with two ports for supplying oxygen for 2 persons at the same time. If more than 1 non-portable oxygen cylinder is used there must be 2 flow meter units for supplying oxygen for 2 persons at the same time.
- One complete portable set with 2litre @200 bar of oxygen ready for use and a spare cylinder of 2litre@200 bar.
- All other vessels that do not have to comply with the MFAG are only required to carry a 2litre@200 bar portable oxygen set, and a spare cylinder of 2litre@200 bar.
Storage of Medical Oxygen Cylinders The Ship Registry considers that the storage of large quantities of oxygen in an accommodation space is potentially dangerous and that it may pose a fire and safety hazard.
In order to resolve the conflict between the intentions of MFAG and the fire and safety issues the Ship Registry recommends that compliance with the MFAG requirements can be achieved by :-
1. The supply of smaller cylinders inside the accommodation
- The required amount (40L@200bar) of medical oxygen in a number of smaller capacity (e.g. 4 cylinders of approximately 10 litres@200bar each, or equivalent) for use inside the accommodation.
- One of the cylinders should be stored in the hospital ready for immediate use. The other remaining cylinders are to be securely stored in a suitable space outside the accommodation, where the cylinders will be protected from deterioration and where the risk of fire and explosion is minimised.
- As a consequence of the difficulty that can be experienced in obtaining and refilling 10 litre cylinders, in the event that a 40 litre cylinder is installed it is recommended the following guidance is used:
2. Use of a single 40 Litre Cylinder
- The use of the 40 litre@200bar medical oxygen cylinder can be stored in either of the following locations:
- Outside the accommodation block, as close to the hospital as is reasonably possible, in a secure and weather protected cabinet.
- Inside the accommodation block in the hospital beside the bed(s), provided the cylinder is securely locked in a frame connected directly to the steel structure of the ship.
- The Ship Registry recommends that a 40 litre oxygen cylinder situated either inside or outside the accommodation block should be fitted with the following safety device to prevent accidental release of high pressure oxygen into the hospital:
- The oxygen regulator in the pipework from the 40 litre cylinder should have a relief valve fitted with a discharge line piped outside the hospital to free air. This ensures that if there is a fault in the system, high pressure oxygen cannot escape into the low pressure side of the system, and will be vented outside of the accommodation.
3. All systems should be maintained and inspected as follows:
- Inspected annually on board by a competent person in compliance with the manufacturer’s instructions.
- Note: a competent person may be a senior member of the ships staff.
- Medical oxygen has a limited shelf life of 3 years and should be landed ashore for re-charging at the expiry date.
- The cylinders are to be hydrostatically tested every 5 years, or at an interval specified by the manufacturer, whichever occurs sooner.
- Oxygen pressure regulators should be serviced at least every 5 years.
- Grease or oil should not be used to lubricate high pressure oxygen fittings.
- All high pressure pipes from the bottle to the regulator should be subject to a pressure test every 3 years by the manufacturer or his appointed gents.
- The hospital ventilation system should be maintained as per the manufacture’s instructions and operating correctly at all times.
- There should be a warning sign on the hospital door stating ‘high concentrations of oxygen may be present’.
- There should be a sign in the hospital adjacent to the oxygen installation stating, ‘all system valves to be shut when not in use’.
Oxygen resuscitation kitsValve and bag oxygen resuscitation kits are primarily applicable to people who are not breathing. They are intended for use only by trained persons. There are a number of manufacturers marketing these products and training must be related to the manufacturers’ instructions relating to the specific model carried on board.
The basic parts of the kit need to be stored assembled correctly in accordance with the manufacturers’ instructions and ready for use. Generally they comprise:
- Face mask (sizes varying depending on the size of the face, but for adults usually there are only two sizes, large and small).
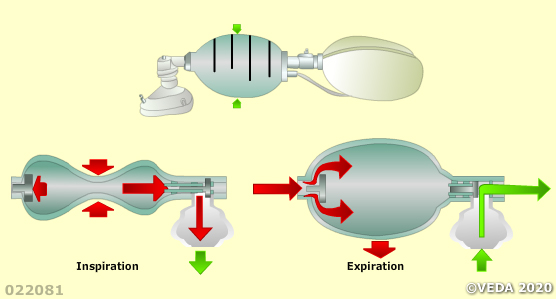
- a) The bag with valve to which the oxygen intake is attached,
- b) The oxygen reservoir also attached to the bag and valve.
The oxygen supply needs to comprise:
- A cylinder containing medical oxygen (industrial oxygen may contain unsafe impurities).
- A reducing valve with wheel control.
- A pressure gauge and valve with “on” “off” knob.
- Hose connecting the bag to the “on” “off” knob for the valve.
Note: When the kit is operating successfully, oxygen will be heard to be flowing through the tubing. If the cylinder is empty or there is a kink in the oxygen supply tube, the casualty receives air only (21% oxygen). But this is similar to giving ordinary mouth-to-mouth ventilation.
Oxygen for the casualty who is not breathingIf the casualty does not have a pulse or heart beat, CPR should be performed immediately by a second rescuer. Administration of oxygen as soon as possible is critical.
A Guedel airway should be inserted. If insertion of an airway cannot be achieved, the chin should be pulled forward throughout the administration of oxygen. If the casualty has seizures due to the lack of oxygen, administration of oxygen may be difficult but is essential.
Use a positive-pressure manual operated oxygen resuscitator in accordance with manufacturer’s instruction. It makes assisted or controlled ventilation possible.
Oxygen should be used at a flow rate of 8 litres per minute. The bag should be squeezed steadily and firmly and released about 12 times a minute. As the bag is squeezed, watch the chest rise and listen for the sound of escaping air which indicates that the face mask seal needs adjusting. It is essential that the face mask is held firmly in place so as to avoid leakage.
If gagging occurs, remove the airway. Always maintain a regular check on the pulse in the neck. The absence of a pulse indicates the need for 15 chest compressions to every two inflations. Once the casualty is breathing spontaneously, put him in the recovery position.Oxygen for the casualty who has difficulty in breathing
- Make sure difficulty in breathing is not due to airway obstruction (see appendix 2).
- The casualty should be connected to an oxygen-giving set through a simple disposable face mask (non-venturi type) placed securely over the face.
- Oxygen should be used at a flow rate of 6 to 8 litres per minute (see appropriate table for recommended setting).
- Oxygen should be continued until the casualty no longer has difficulty in breathing and has a normal healthy colour.